Is Stevie saying, “SNIPPED?”

Is Stevie saying, “SNIPPED?”

In men with prior vasectomy, microsurgical reconstruction of the reproductive tract is more cost-effective than sperm retrieval with in vitro fertilization and intracytoplasmic sperm injection if the obstructive interval is less than 15 years and no female fertility risk factors are present. If epididymal obstruction is detected or advanced female age is present, the decision to use either microsurgical reconstruction or sperm retrieval with in vitro fertilization and intracytoplasmic sperm injection should be individualized. Sperm retrieval with in vitro fertilization and intracytoplasmic sperm injection is preferred to surgical treatment when female factors requiring in vitro fertilization are present or when the chance for success with sperm retrieval and intracytoplasmic sperm injection exceeds the chance for success with surgical treatment.

The question on vasectomy.com is about IVF however a microscopic reversal is also a reasonable option in this scenario.
It takes two to tango but only one testicle to conceive!
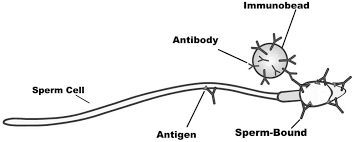
Antisperm antibodies were measured in serum and seminal plasma in 130 males before and after vasectomy reversal and the occurrence of pregnancy was analysed in the partners of 77 who were followed for more than one year. Sperm-agglutinating antibodies were found in the serum of 79% of patients; seminal plasma antibodies were present in only 9.5% before reversal and this rose to 26% afterwards. Pregnancies occurred in the partners of 53% of those men who were trying to produce children. A pregnancy was significantly less likely when the pre-operative serum antisperm antibody titre was 512 or more, but no decrease in fertility was seen with titres below this. Several pregnancies were produced by patients with seminal plasma antibodies, but numbers and follow-up are too small to permit detailed analysis.
A randomised controlled trial of peri-operative steroids showed that they produced no benefit.
The antisperm antibodies associated with vasectomy reversal appear to differ fundamentally from those occurring in naturally subfertile males.
Article Reviewed: Outcomes for Vasectomy Reversal Performed After Obstructive Intervals of at Least 10 Years. Kolettis PN, Sabanegh ES, et al: Urology 2002; 60 (November): 885-888.
A lot of couples debate which of the two major methods of having a child after vasectomy they should pursue. Often times it is a decision based on cost. For that couple wanting to do IVF first, this study shows no significant scarring as a result of the aspiration and no significant negative effect to a successful vasectomy reversal.
Urology – July 30, 2008 – Vol. 24 – No. 07
Article Reviewed: Results of Vasovasostomy or Vasoepididymostomy After Failed Percutaneous Epididymal Sperm Aspirations. Marmar JL, Sharlip I, Goldstein M: J Urol; 2008; 179 (April): 1506-1509.
